.png)
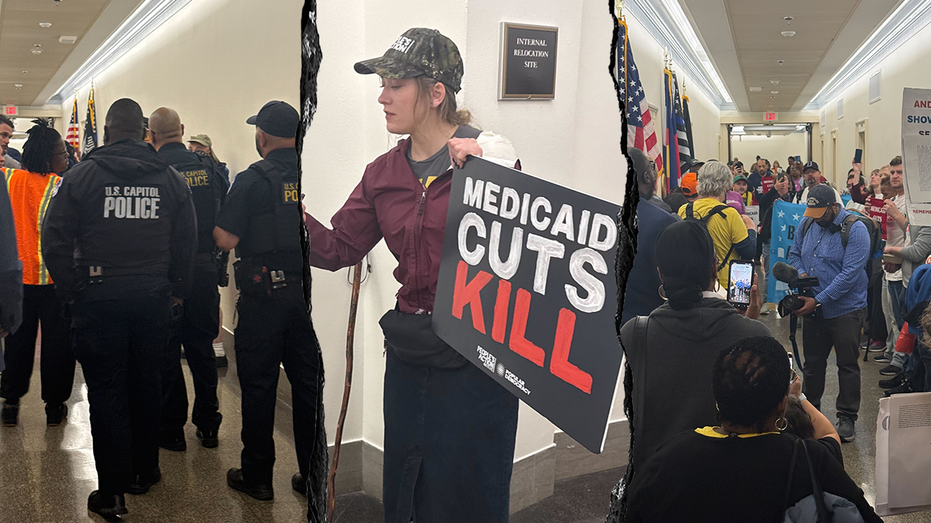
As Republicans have labored to craft President Donald Trump’s domestic policy megabill, conservative hardliners have been eager to slash spending on Medicaid, which many of them see as riddled with fraud and abuse. One target in particular for the right: the wonky, but hugely important, topic of provider taxes.
Conservative GOP lawmakers and think tanks accuse states of using taxes levied on hospitals as a loophole to get more money from the federal government — a practice they say is akin to legal “money laundering.” The legislation, which couldsee a vote as soon as Wednesday, would freeze current provider tax rates and place a moratorium on any new provider taxes.
The proposal has drawn stiff blowback from hospitals and states, which use revenue from the taxes to pay for their share of Medicaid payments and make hospitals whole through higher payments. Red states — and Trump voters — in particular might suffer.
“It is a real problem if you change these programs without thinking through how they affect rural communities,” said Alan Levine, who previously led health agencies in Florida and Louisiana under Republican governors and now serves as president and CEO of the hospital system Ballad Health, which has rural hospitals across parts of Appalachia.
In an interview with POLITICO Magazine, Levine argued the taxes are not a scam, but a tool for states to help rural and underserved hospitals with high Medicare and Medicaid populations that already run on thin margins. The revenue can help offset losses from high care denials initiated by privately run Medicare Advantage plans.
Levine also discussed what he learned fighting Medicare and Medicaid fraud in Florida, and why he thinks the debate isn’t over, even if this bill does eke its way to House passage.
This conversation has been edited for length and clarity.
You led top health agencies for two different red states. You’re now concerned with what Republicans in Congress are proposing for Medicaid. Why?
My concerns aren’t necessarily with what Republicans have been doing in Congress. My concerns have been individuals who have characterized legitimate and legal funding mechanisms for Medicaid to be something they are not.
Forty-nine different states use provider taxes as a mechanism for coming up with a state match to fund their Medicaid programs. While certainly there are states that the evidence shows have stretched and abused it, most states that I am aware of that use these mechanisms do it to keep access to rural hospitals for underserved communities.
Referring to this process as money laundering is simply not fair. It implies that something illegal and nefarious is being done and that is not true.
Governors have got to be entrepreneurial, thoughtful and innovative in terms of how they utilize these federal funds to keep access available.
Since 2016 we saw a huge spike in Medicare Advantage insurers and saw a huge increase in [care] denials. We need help, and states have used provider taxes as a means to offset the loss of these Medicare dollars. They are trying to draw down federal dollars in Medicaid to make up for the loss of federal dollars in Medicare.
I think there’s a clear recognition by Congress that these mechanisms have been there for a long time and you can’t just take a sledgehammer to them. The current bill as it relates to this funding mechanism puts a freeze on it, and that is probably a good start if you are going to evaluate how these programs are being done in the future.
We’re a rural system. You have a disproportionate number of patients covered by Medicare and Medicaid. It is a real problem if you change these programs without thinking through how they affect rural communities.
Can you tell me a little about the dynamic between privately run Medicare Advantage plans and your hospitals? I know some hospital systems have clashed with the plans over how to set payment rates.
Our quarrel with Medicare Advantage insurance companies is not over rates. It is over behavior.
Let’s say our rates for a Medicare Advantage insurer are 100 percent of traditional Medicare fee-for-service. When you net out what we get paid because of the denials and unilateral downcoding such as shifting a patient from inpatient to outpatient, we are generating 85 percent in the aggregate of what we get from traditional Medicare.
That is a 15 percent cut for the hospital.
I don’t think Medicare Advantage is a bad thing. I do think the behavior of the insurance companies — and they are not all the same — is to take the premium and then systematically not pay claims.
It affects hospitals that have a disproportionate number of low income patients because you can no longer afford to pay them.
Going back to the House bill, it proposes a moratorium on new provider taxes. How is the moratorium going to impact Ballad’s hospitals? Is that the right policy to pursue?
It could impact our hospitals, but I don’t know yet. There are still things going on in Washington with respect to Tennessee’s Medicaid program that remain undecided.
In theory the freezing of it based on the language of the bill would not hurt Tennessee, which is a positive thing.
I don’t think this bill will be the last of the conversation. I think there will be more discussions about the use of provider taxes going forward.
The megabill proposes a similar restriction for state-directed payments. The practice enables states to direct how providers are reimbursed by a Medicaid managed care plan, which is a private plan that oversees the Medicaid program for a state.
The bill would restrict any state-directed payments above the Medicare payment rate, as some of the payments can be made at commercial rates. Does Ballad rely on these state-directed payments?
We are 100 percent managed Medicaid. Any time a state wants to implement a payment policy they have to use state-directed payments so the insurance companies can pass the dollars through.
The problem with tying the payment rates to Medicare is the Medicare policy by design disadvantages rural areas. The Medicare area wage index, which adjusts Medicare payments by geography, severely disadvantages rural and non-urban areas.
If you tie state-directed payments to Medicare rates you are [hurting] rural hospitals yet again because the wage index applies to that.
One of the biggest policy changes in the bill would be to impose new work requirements for able-bodied Medicaid recipients, leading to 4.6 million people potentially losing insurance through 2034. Are you concerned about people being dropped off Medicaid and how can you prevent that?
When Democrats say work requirements mean people won’t be able to access care, that generally is not true. As a not-for-profit health system, we are required to have a charity policy. For us if you make 225 percent of the poverty level you get your care for free from Ballad.
The lowest threshold I have ever seen in a hospital for charity care is 150 percent of poverty. We tend to run higher due to the demographics of our region, but 150 percent of poverty is above the eligibility threshold for Medicaid.
The reality is that people who lose their Medicaid coverage because they are not working can still access medically necessary care if they have not-for-profit hospitals available to them. What is also true is we are going to provide the care and the cost is still going to be incurred, it’s just that we are eating it. The cost of care exists no matter what, it is just who is going to pay for it.
In your previous roles in Florida and Louisiana can you share what you did to combat waste, fraud and abuse in health programs?
In both states I worked collaboratively with the attorneys general and cracked down on Medicaid fraud. When you see the cleverness of the criminals and thieves inside these programs it is amazing. They are obviously very smart and very calculating.
A lot of our efforts were using computer mechanisms and technology that is ancient compared to what they have today. We would try to find patterns where, for instance, a new provider enrolled in the program and within a month is billing a million dollars a month.
To the naked eye when you are processing 160 million claims a year it is not easy to catch that.
With the use of technology, which I think [CMS Administrator Mehmet] Oz is committed to, I think you can catch a lot of those schemes and get those bad players out of the program.
What was the most egregious case that you saw?
Oh my gosh. I won’t say this is the most egregious, but this is an example of how this [fraud] can happen.
This was in Florida. We were finding children who needed wheelchairs, and two-year-olds were given wheelchairs that cost $50,000 to $60,000 with off-road technology and certain types of adjustments. Why is this happening?
What we found was the wheelchair manufacturers were the ones deciding which types of wheelchairs these kids needed. It was the fox watching the hen house.
I will never forget when I had my confirmation hearing in Florida and 30 children in wheelchairs showed up to protest my confirmation. We found out a public relations firm was hired by the wheelchair manufacturer to prearrange having those kids there to protest me. That is what you are up against.













 English (US)
English (US)