.png)
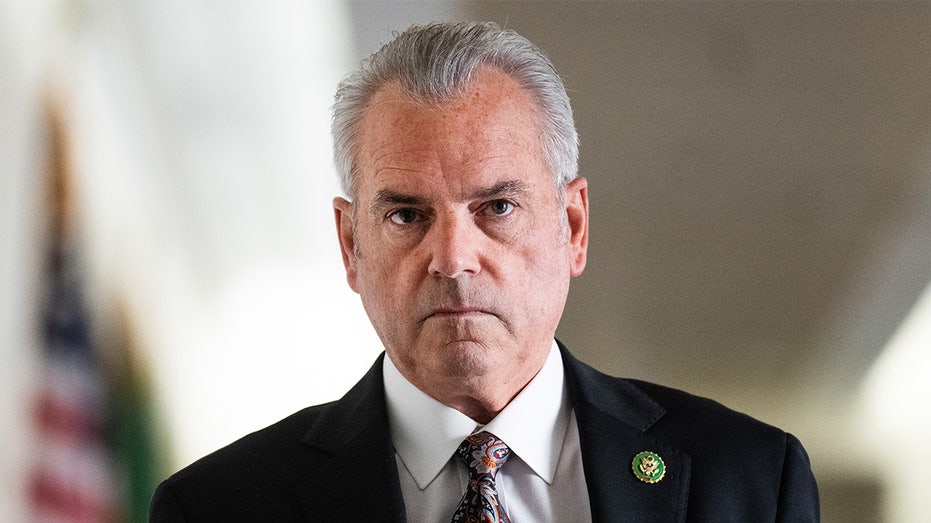
Jay Bhattacharya is no longer on the fringe.
When the Covid-19 pandemic hit, the then-Stanford professor was one of the loudest critics of lockdowns, school closures and what he called “utopian” public health planning, and he was often dismissed by mainstream public health officials.
Five years later and Bhattacharya is now the director of the National Institutes of Health, one of the most powerful figures in public health and biomedical research in the U.S. and across the globe. He oversees a budget in the tens of billions and helps determine who gets funded — and whose ideas get left behind.
“The first and most important thing,” he says in a new interview with POLITICO Magazine, “is that dissenting voices need to be heard and allowed.”
In a wide-ranging conversation, Bhattacharya laid out his vision for American science under President Donald Trump and discussed the ongoing fallout from the pandemic. In particular:
- He praises the pardon of Anthony Fauci even as he effectively accuses the former public health official of engaging in a Covid cover-up.
- He endorses the creation of an independent commission to assess the pandemic response.
- He rejects the continued recommendation of mRNA vaccines for healthy young people — and says he himself has received just two doses, both in 2021.
- He explains why he thinks it’s unlikely vaccines cause autism — but that he won’t prejudge the issue.
- He waves off the notion that Europe would be able to poach American scientists amid Trump’s war on elite universities. “France is a nice place to visit,” he scoffs.
This interview has been edited for length and clarity.
You’re one of the strongest critics of America’s and the world’s Covid-19 response. You’re an outsider that politicians didn’t really listen to. Now you’re in charge of NIH. What would a better response look like next time if there’s a next pandemic?
I think, God willing, there’s no next time. But I think the first and most important thing is that dissenting voices need to be heard and allowed.
It’s never going to be appropriate for the government to suppress opinions in thinking about how to manage a pandemic. I think that if just that one thing had been done, a lot of harm could have been avoided. Beyond that, we also need to apply the precautionary principle correctly. You’re allowed to assume the worst very early in the pandemic about the disease.
This is what happened.
Absolutely. I think that was actually appropriate very early. When it’s potentially catastrophic, you’re allowed to assume the worst. What you’re not allowed to do is assume the best about your interventions. You can’t assume that the interventions you deploy are automatically going to work. That’s not part of the precautionary principle. You still need to do a careful analysis.
You need to understand the harms of the interventions that you’re imposing and make decisions on the basis of that. You know that if you close schools for extended periods of time, you’re going to harm children at scale, which is exactly what we did.
That was one of the most important measures that were taken — not only in the U.S.
Yes. Germany closed the schools and Sweden didn’t — and you see that Sweden ended up doing better than Germany.
The third thing I think you need to do is you need to identify the most vulnerable people and work to protect those people. A society-wide response, like we saw in 2020, cannot possibly succeed because societies are deeply unequal. The capacity for people, especially poor people, to comply with the kinds of orders that were put in place in 2020 are fanciful. The world’s poor cannot abide by another lockdown. You have to focus on the achievable, not on fantasies based on computer modeling.
So you’re saying all this didn’t happen during the Covid pandemic. Why wasn’t an approach like this taken?
I can only speak from the scientific point of view. The policy point of view I can only speculate on. Scientists at the very top of the public health and scientific institutions of the world decided that they knew best how to manage the pandemic. And they decided that they were going to drown out dissenting voices.
Which institutions are you talking about?
I mean the institution I’m leading for instance, the National Institutes of Health, the equivalent in Germany and the World Health Organization. They convinced governments around the world that the only way to save lives was to follow the lockdown path and that they needed extraordinary, almost dictatorial powers, suppressing free speech, suppressing freedom of movement, suppressing the principle of informed consent in medical decision-making, controlling nearly every single aspect of society, designating who’s essential and who’s not essential, closing churches, closing businesses.
And they made this decision for the whole world whether it was a poor person living in the Congo or Uganda or India or the Philippines — or a rich person living in Beverly Hills. The idea was the same: lock down everything. As a result, poor people were hurt everywhere. We shut down measles and other vaccination efforts in Africa in favor of Covid control, even though measles is a much worse disease for Africans than Covid.
All this — what does it mean for trust in institutions, trust in science? How do you look at this, a few years after the worst of the pandemic?
I think it’s been catastrophic for the public perception of scientists. It’s heartbreaking to look at. I looked at a Pew poll from 2024. I think the estimate was something like one in four Americans placed no trust at all in scientists to do what’s in the public interest. That’s a shockingly high number.
Should there be a formal, independent commission — like after 9/11 — to assess the pandemic response and assign responsibility?
Well, I’ve argued for such a commission before I was NIH director. I think it would be helpful to have an honest look at what happened in 2020. The goal of such a commission is not to place blame, but to assess the mistakes and then change our processes so we don’t make those same mistakes again. The model of such a thing I have in my mind is something like in medicine, after a patient dies unexpectedly in a hospital. What will happen is something called a morbidity and mortality conference, where everyone involved in the patient’s care will get together and say, “Well, here’s what went wrong.” The goal is to find out why what happened happened — and then learn from it so that the next patient doesn’t face the same problem.
It’s probably quite hard to achieve this in the U.S. and other countries, considering the emotional nature of the debate.
I think the time is coming. Initially, I thought in 2021 and 2022 that people would be open to it. I was very naïve. I became somewhat depressed about this possibility of a commission of some sort or an honest look at the mistakes of the pandemic in 2023-2024. But I think things are starting to open up. People, I think, are much more willing now that they see the harm that has been done to kids. And there is also the continuing levels of depression and anxiety, the high levels of drug abuse and drug overdoses, the economic damage.
At the same time, there are calls to prosecute Anthony Fauci and others. How do you see this? You’re saying the goal isn’t blame — but to be better prepared. Yet there’s a lot of blame being assigned.
Yeah. I don’t want to participate in those blame games. I disagreed with a lot of what President Biden did, but I thought his pardoning of Tony Fauci was a wise thing. But my preference for diffusing the personal attacks shouldn’t be taken as a desire to not have an honest, frank discussion about the mistakes of the pandemic.
Do you believe the U.S. — or other countries — should do more to uncover the origins of Covid-19?
Yes, but I think the Chinese need to cooperate and they have not cooperated.
The World Health Organization sent a mission there which wasn’t successful at all.
Yeah, I think it’s impossible to make a country like China cooperate unless they want to. There’s enough evidence that I’ve seen from the outside that suggests that there was at the very least a cover-up of dangerous experiments that were done in China with — by the way — the help of the U.S. and also Germany and the UK.
There was an international effort to try to supposedly prevent pandemics by finding viruses and pathogens in the wild, like in bat caves, for instance, in southern China, bringing them into labs, making them more transmissible to check if it was possible to cause a pandemic. I think that was a very, very dangerous kind of utopian research agenda.
I’m convinced that research agenda led to this pandemic through a lab leak in China, in Wuhan.
But that was a global effort.
Very early on — in February 2020 — scientists and high-ranking officials were already labeling the lab-leak theory a conspiracy.
I think that was a part of the cover-up.
It’s absolutely striking that leaders like Tony Fauci would spend so much time trying to say something like, “Look, it can’t possibly be a lab leak, this is a conspiracy theory,” trying to suppress the idea, denigrating scientists who very legitimately raised this possibility — these are not actions that scientific agencies ought to be taking.
You’ve publicly clashed with the famous German virologist Christian Drosten. He called you and the other authors of the Great Barrington Declaration, which opposed lockdowns, “pseudo-experts.” What’s your response?
Well, I think it’s unfortunate that someone like Christian Drosten will throw names around rather than trying to engage with reality. My expertise is in epidemiology, in health policy. Understanding the consequences of actions like the lockdowns on the global poor is squarely within my expertise. When we’re considering such a large-scale response, to say you must be a virologist to understand what to do is a tremendous mistake.
There are huge impacts of policies like lockdowns, and you need a wide range of scientific expertise to understand both whether they are likely to be efficacious, what consequences they’ll have and how to mitigate some of those consequences. Virology itself is not enough.
But politicians and decision-makers were listening to him — and not to people like you.
I was just a Stanford professor. I was a fringe epidemiologist. Why would anybody listen to me?
Would you be willing to debate Drosten — or others you’ve criticized — in a public forum?
I’ve engaged in scientific debates throughout the pandemic including with people on the other side, beyond the lockdowns, on much else, on vaccine mandates, on free speech. So yes, I’d be delighted.
The White House has proposed cutting the NIH budget by 40 percent. Is a cut that deep possible without damaging important research?
I want to put this in context. As I said, the public has a distrust now for science and scientific agencies. And based on what we’ve discussed up to now, you can sort of understand why. At the same time, the scientific work we do is very important for the health and well-being of the public. President Trump has issued a letter to Michael Kratsios, his chief science adviser, committing that the U.S. government will take actions to make the U.S. the world leader in biomedicine in the 21st century. He’s made commitments to Secretary [Robert F.] Kennedy [Jr.], the head of Health and Human Services, my boss, that he will take actions so that we can make America healthy again. And the NIH is now, and will be in the future, a vital part of that.
And the cuts?
The budget proposals that you’re talking about are a beginning of a negotiation between Congress and the White House. I don’t want to get in the middle of that negotiation, so I shouldn’t comment too much on that specifically. I’ll wait to see what the final budget looks like.
But even if we can’t talk about the result of the negotiations yet, are there really billions of dollars’ worth of wasteful research at the agency?
Well, that’s a difficult question to answer because you’d have to make a judgment on scientific processes and research that takes sometimes decades in order to understand what the full impacts are. That said, there’s no question that there’s things that the NIH was doing that it shouldn’t have been doing, that needed to get reduced.
What comes to your mind first, now that you’ve been in office for a few weeks?
Probably the most important example is something that the president just issued an executive order about. He ordered that dangerous gain-of-function research not be conducted, not be supported by the U.S. government, certainly not by the NIH. Work that has the potential to cause a pandemic is something we should not be doing and we’re not going to now that the executive order has been issued. Money spent on that was not money well spent. There are other kinds of research priorities that previous NIH directors had that I think were not advancing science.
Cutting programs on diversity, transgender care and women’s health?
Yes, I do want to talk about that. And I want to talk about that in a very specific way. But first by setting up the principles, right?
Sure.
The first principle in this discussion is that the NIH has as its mission the research that advances the health and longevity of all Americans, meaning everybody. It doesn’t matter what your race is, it doesn’t matter what your age is, it doesn’t matter what your sex is, it doesn’t matter what your sexual orientation is. It doesn’t matter who you are. If you are a human being, and especially if you’re an American human being, I’m very interested in supporting research that advances your health.
But what about transgender studies?
Even for folks who are considering transgender surgeries or hormone blocking, I want to understand what the health consequences are so that we can give you the best scientific advice about that. The question is one of prioritization. You have to make decisions about which projects are most likely to advance health.
You don’t want to ignore rare conditions. But at the same time, American life expectancy has been flat since 2012. We haven’t made advances in health. We have not fulfilled our mission of advancing, of doing the research that at least translates over into expanding health status.
German life expectancy, for example, has gone up since 2012. Why has the United States life expectancy not?
We have to focus on — and I don’t think we have focused on it enough — the diseases and conditions that impact the broad numbers of Americans. We have made no progress on obesity until very, very recently. Type 2 diabetes, strokes, Alzheimer’s, autism. On condition after condition after condition, there are millions of Americans, tens of millions of Americans, hundreds of millions of Americans who are suffering. And our obligation is to provide the research that improves their health.
So that’s the first principle.
The second principle is that we want to focus on real scientific ideas that actually improve health. So, I want to distinguish that from ideological constructs like DEI that in many ways are not even in principle falsifiable. If you believe structural racism is the primary reason why minorities are in lower health, how would you disprove that? What experiment could you do to disprove that? If you can’t think of an experiment to disprove something, then that’s not a scientific idea.
So you’re saying diversity, equity and inclusion, DEI, is not a scientific idea?
I mean, we could get into some specifics and maybe it would help. One specific might be the hypothesis that structural racism in the United States, however we define it, is the cause of lower life expectancy for Black Americans in the United States.
Now, that’s a hypothesis as stated, right? It sounds like a scientific hypothesis. But can you imagine any experiment that would in principle lead you to reject that hypothesis? And I think the answer is no. It’s not in principle possible to think of an experiment that would lead you to reject that hypothesis. If the answer is no, then it is not actually a scientific hypothesis.
Another aspect of it is the intervention that you’re envisioning, is it even a feasible intervention? How would you reverse all structural racism to improve minority health? Is it really the most important contributor to why Black Americans live shorter lives than white Americans?
It seems to me that it’s better to address the actual health problems that Americans have, whether people are white or Black: How do you treat type 1, type 2 diabetes? How do you prevent obesity or manage obesity? How do you prevent kidney disease? How do you prevent strokes and heart attacks? How do you manage them better? Those things actually impact the lives of Black Americans.
Those things result in countless suffering, and useless fights over structural racism — something that the NIH is not well equipped to reverse because I’m not even sure how it would be possible to do — is not something the NIH can constructively do. It seems like a waste of resources.
The administration recently told Harvard University that it’s disqualifying the school from receiving additional federal grants. As a former Stanford professor who was penalized for holding non-conformist views, do you see this as collective punishment?
First, the NIH makes distinctions based on the policies and the capacity of each institution to support excellent research. The administration has found that Harvard engaged in actions that made research very difficult to do there — civil rights violations that led Harvard to lose a Supreme Court case over racially biased admissions. And I can tell you that I had a colleague at Harvard, Martin Kulldorff, who faced tremendous difficulty in expressing his scientific ideas, in part based on the policies that Harvard followed.
Second, I believe that Harvard has produced a tremendous amount of great research over the years with a huge number of excellent scientists.
And so third, there is a possibility — and I hope very, very soon — of a negotiated deal where Harvard removes the things that make it difficult for free speech to happen on campus, to comply with basic civil rights laws on campus. And once they do that, we’ll be back to a position where Harvard is considered an excellent institution.
But for now, as a researcher at Harvard, you won’t receive any funds if there’s no deal between the administration and the university, right?
I anticipate that there will be a negotiated settlement over this in due time. That seems to make the most sense to me. But it’s going to take a lot of action on Harvard’s part to make that happen. And I think as a researcher, I would encourage the leadership of the university to work toward that negotiated settlement as rapidly as possible.
European leaders have just launched a 500-million-euro fund to lure scientists away from the U.S., amid what one professor called a “libertarian assault on science” under President Trump. What do you make of that?
A libertarian assault on science… Okay, I’m not sure what that means. I don’t think President Trump is any libertarian, and nor am I. I think that the idea that the United States no longer supports science or scientists is laughable. Even if we had that budget cut in the proposal that you talked about earlier, the United States would still be the single largest funder of biomedical scientific research in the world, and it wouldn’t be close.
Salaries of scientists are higher in the United States. Scientific opportunities in the United States are now and will continue to be the best in the world. The U.S. is not going to lose scientists because of some temporary disturbance caused by the change of an administration. The structural factors that make America the top nation in the world in biomedical sciences will remain in place.
The French President Macron said: “If you love freedom, come help us stay free.” So wouldn’t it make sense for a Harvard researcher — who’s about to lose NIH funds — to move to Europe?
I mean, France is a nice place to visit. I love France and I spent some time there myself as a student, but I still think that the United States, if you’re a scientist, is the best place in the world to gain resources, to do the work you do. And then second, to have the capacity to network with other scientists and gain access to materials and ideas.
International competition in science is a long-standing thing going back decades. But I have to say, it’s funny, specifically France, because there are friends and colleagues of mine who had a very difficult time expressing their ideas during the pandemic. It was a pretty bad place to be a dissident scientist in 2020, 2021, 2022. So to say the idea that France has free speech and Europe has free speech when there are European laws to suppress dissent online and where you can have the police come visit your house if you post something that the government doesn’t like online — that doesn’t make sense.
You are mentioning free speech. A few weeks ago, Kevin Hall — one of NIH’s top nutrition researchers — resigned and accused the agency of censoring his findings on ultra-processed food. You’ve said the NIH must never censor scientists. What went wrong?
That happened before I got into office. I got into office in April, and I learned about this Kevin Hall situation a couple of weeks later. I did a few things. First, I invited Kevin to come and talk with me. What I understood happened had nothing to do with any suppression of free speech. I think it was due to a misunderstanding, but it’s a misunderstanding due to a policy that I changed.
What do you mean?
There’s an intramural researcher campus inside the NIH with thousands of researchers, and then we also send grants outside, to Harvard — once upon a time to Harvard — to Stanford, and all the other universities of the world.
In the intramural program, there was a policy that said that if a researcher wanted to publish a paper, they had to get clearance from their supervisors in order to send the scientific paper out. Often the clearance would include consideration of substantive factors, and they would ask the researcher to change their paper. Now, I have some criticism of Stanford’s policies on free speech during the pandemic, but for at least 20 of my 25 years at Stanford, I never had to get permission to send my paper out for review to a scientific journal. Academic freedom means I can send my paper out even if my bosses disagree with me.
So what does this mean for the case of Kevin Hall?
The policy I mentioned was before his case. And I put in place a policy that says that there is no more review. I established academic freedom for publishing scientific papers on the NIH campus so that scientists can publish whatever result they like in scientific journals. They have to say that they’re speaking for themselves, not for the NIH, of course, but that’s just normal. I don’t know if that’s for the first time ever, but it certainly reverses the earlier practice that I found when I first arrived on campus. In fact, I offered Kevin Hall to come back.
What did he say?
He’s considering. I thought he accepted it already, but then I learned he hasn’t. He’s still considering it.
You’ve found support from both Trump allies and RFK Jr. backers. Where do you stand between those two camps?
The alliance between the Trump supporters, the MAGA, and the Bobby Kennedy supporters, MAHA, it’s actually an incredible alignment. And I’ll tell you why. I think President Trump, whatever you may think of him, he speaks for the regular person, right? His concern for regular people, the well-being and the livelihood of regular people is just very, very clear. How can they live healthy lives? How can they avoid the chronic conditions that leave them unable to enjoy their lives to the fullest? Bobby Kennedy, he spent decades wanting that. He’s told me, and you can see it, he’s sacrificed a lot so that he can be in a position where he can help make America healthy because he cares about the health and well-being of regular people. I find that very, very attractive. I find the commitment to the lives and well-being and health of the vulnerable, of the working class, of regular people, a really attractive goal. I can understand how it was such a popular political agenda.
One of the most controversial initiatives of the new administration is the plan to investigate the causes of autism. What do you want to find out?
I want to know what’s caused the rise in autism. I want to work with the autistic community to understand what their concerns are. I mean, I know from my own personal life and friends and family, the very wide range of presentations of autism.
There may be people who are very good, kids who are very high-functioning, very smart with the autistic label. Then there’s families that are affected with much more, with kids that have many more disabilities, severe disabilities. There are countless hypotheses of trying to understand why autism rates are so high as measured in the U.S.
The CDC said it was 1 in 31. I want to understand the biology. And I want to understand the variation across different regions in autism. Are there environmental exposures that are at play? Is it things that happen during pregnancy?
As a scientist, I don’t know the answer. If someone were to ask me what causes autism, I don’t know the answer. It’s not just a matter of curiosity for me. I want to help my friends who have autistic children better understand how they can help their kids.
Do you personally think vaccination could be a cause of autism?
Some vaccines have been studied extensively for a link to autism, like the MMR vaccine, and scientists have failed to find it in really well done studies. It seems unlikely for MMR. Others have not been as well studied. As a scientist I’d say it’s unlikely that one of the vaccines is the cause but I don’t know for certain.
What I do know is that if I prejudge the issue in advance, I’m very likely to have a blind spot. And certainly people may not trust my answer.
I don’t know what it’ll end up being. People will accept that if all possible hypotheses are entertained. That’s the reason to include that among the set of hypotheses, because if you exclude that as a hypothesis people won’t believe the answer.
RFK Jr. is reportedly reviewing NIH contracts related to mRNA vaccines. What’s your own view on their safety and efficacy?
Well, I think there’s some well-known safety signals, negative safety effects of the mRNA vaccines. In particular, I don’t think anyone disputes that it increases the rate of myocarditis, especially in young men. And there are other safety signals that have been identified.
Focused on the Covid vaccine, it’s a very different place we’re in now than in 2021. Most of the population has had immunity to Covid because of prior infection. Randomized trials that were done in 2020 on the vaccines in a mostly immune naive population don’t necessarily translate over to now.
And yet we do know that there are those side effects. So especially for healthy young people it makes no sense to me to continue to recommend the vaccine. It’s time to revisit. The mandates and the passports and the pressure to have everyone take the vaccine soured people on the platform.
Many, many people now think that mRNA is a bad platform. And I think that it’s really that government pressure which violated the informed consent rights of so many to take the vaccine. There was the promise that you wouldn’t get Covid if you are vaccinated, but then of course, it didn’t stop you from getting Covid.
Those things together made the mRNA platform a difficult platform to use from a pure, wide-scale public health perspective going forward. The manufacturers are going to have to find some way to address that widespread public skepticism about the platform.
What about the NIH director? Is he up to date with his Covid vaccines?
I don’t know what up to date means but I’ve had two versions of it, two shots of it in, I think, April and May 2021, and I have not had any since.













 English (US)
English (US)